










A new Canadian guideline on the management of adult obesity looks at root drivers and overall health
A Canadian clinical practice guideline for treating adults with obesity puts an emphasis on improving overall health and managing obesity as a chronic disease by addressing its root drivers.
A summary of the guideline, which was developed by Obesity Canada and the Canadian Association of Bariatric Physicians and Surgeons, was published online August 4, 2020 in the Canadian Medical Association Journal. The guideline assessed more than 500,000 peer-reviewed articles, made 80 key recommendations, and, of particular significance, is bookended with chapters devoted to weight bias and the care of Indigenous people. The issue of obesity management clearly resonates with many physicians as the summary was the most read CMAJ article in 2020.
Despite growing evidence that obesity is a serious chronic disease, it is not effectively managed within our current health system. Many physicians report feeling ill-equipped to support their patients with obesity, said Dr. Sean Wharton, lead co-author of the study, and an Ontario internist with a focus on obesity management and diabetes.
Importantly, the guideline, which was last updated in 2006, stresses that clinicians need to move beyond simplistic approaches of 'eat less, move more,' — advice Dr. Wharton likens to the treatment of depression in the 1950s, which simply prescribed fresh air and nature walks — and focus on the societal and often systemic determinants of weight and health.
“What we have been doing is not working. We so desperately needed a new approach,” said Dr. Wharton, an adjunct professor at McMaster. The calorie-counting approach, he said, has only led to unhappiness on all sides: frustrated physicians who feel speaking to their patients about their weight is futile and shamed patients who feel they have failed yet again.
In treating obesity as a lifestyle choice, one characterized by laziness and lack of willpower, Dr. Wharton said a huge disservice has been done to patients, leaving many feeling like they have been shut out of the health-care system.
And if there is a population that can’t afford to be receiving marginal care, it is patients with obesity.
Health Complications
The health complications arising from the disease are many. Most concerning, it increases the risk of developing cardio-vascular disease and cancer, two primary causes of premature mortality in Canada that result in a reduction of life expectancy by six to 14 years. It is estimated that 20 percent of all cancers can be attributed to obesity, independent of diet. Obesity increases the risk of colon, kidney, esophageal and pancreatic cancers in both sexes, and endometrial and postmenopausal breast cancers in women. Obesity also increases the risk of developing type 2 diabetes, gallbladder disease and gout. And as of 2020, COVID-19 has been added to that long list, with studies showing obesity is a risk factor for serious illness or death from the coronavirus, particularly for younger patients.
Obesity, said Dr. Wharton, needs to be managed for what it is — a complex, progressive and relapsing chronic disease. “Physicians need to support their patients with obesity with the same compassion and empathy that we manage our patients who have diabetes or hypertension.”
Recognition of obesity as a chronic disease in its own right, rather than simply a risk for other conditions, is very new. It was only in 2013 that the American Medical Association recognized it as a disease state with multiple pathophysiological aspects, requiring a range of interventions to advance obesity treatment and prevention. The Canadian Medical Association followed suit two years later with its own nod.
This recognition on the part of the associations was prompted by research that provided a deeper understanding of the genetic, metabolic, environmental, and behavioural factors that contribute to obesity. Given the last guidelines on obesity management was produced in 2006, these important advances made the release of the guideline timely and necessary, said Dr. Wharton.
Among the insights reflected in the guideline is a relatively recent appreciation of the tenacity with which the body will fight to regain any weight loss, making maintenance virtually impossible for any patient who tries to keep weight off without interventions.
“Physicians need to support their patients with obesity with the same compassion and empathy that we manage our patients who have diabetes or hypertension.”
“Although a caloric deficit is required to initiate weight loss, sustaining the weight loss in the long term is unbelievably difficult due to compensatory mechanisms that promote positive calorie intake by increasing hunger and the drive to eat,” said Dr. Wharton. “That is why taking the approach of restricting calories leaves patients doomed to near certain failure in the long-term,” said Dr. Wharton. The restriction triggers a cascade of metabolic and neurohormonal adaptive mechanisms that ensures patients put on even more weight than before they started a diet.
In fact, Dr. Wharton said pains were taken to avoid using the word “diet” in the guideline — a word loaded with potential negative connotations — preferring instead to call the chapter pertaining to food intake as “medical nutritional therapy,” a phrase that provides clarity that obesity is a medical condition and requires a nutrition plan in line with a medical condition. The advice in this chapter states there is no one-size-fits-all eating pattern for obesity management and adults living with obesity should consider nutrition intervention options that are focused on achieving health outcomes for chronic disease risk reduction and quality of life improvement, not just weight changes. For example, a patient with diabetes may want to use a “low carbohydrate eating pattern,” while a patient with heart disease may rely on a “Mediterranean dietary pattern.”
But before medical nutrition therapy is even explored, the guidelines suggest the issue of obesity be broached with sensitivity. “Empathy and compassion are everything,” said Dr. Wharton. Given the dominant cultural narrative about obesity as a self-inflicted state, there needs to be recognition that most patients with obesity will very likely have had, at some point in their past, a negative experience in a doctor’s office.
Therefore, it is important that, as a first step, doctors ask patients for permission to discuss weight (e.g., they can ask, "Would it be all right if we discussed your weight?") — which demonstrates empathy and can help build patient-provider trust. It also recognizes not every person with a larger body has obesity. If the person’s weight is not affecting their medical, functional or psychosocial health, then the conversation need not go any further.
“This takes the focus off of esthetics and puts it onto health.”
It is also recommended that permission be asked before conducting anthropometric measurements. The calculated body mass index (BMI) and measured waist circumference (WC) are the most widely used measurements, and researchers suggest they be used together to better evaluate health. "Although BMI is widely used to assess and classify obesity (adiposity)," they wrote, "it is not an accurate tool for identifying adiposity-related complications." While the correlation between BMI and body fatness is fairly strong, two people who have the same BMI can have different levels of body fatness. For example, Blacks generally have less body fat than Whites, and Asians tend to have more body fat than Whites.
The guideline authors recommend assessing a patient’s disease severity using the Edmonton Obesity Staging System (EOSS), a five-stage method to classify obesity based on physical and psychological measures, and any metabolic weight-related health problems, such as high blood pressure or obstructive sleep apnea. The patient’s own health goals should also be included when developing an obesity management plan, the authors said, with the target of a positive health outcome rather than a number on a scale.
If the patient agrees to exploring the issues, the physician should also obtain a comprehensive patient history to identify the root drivers of obesity (which could include genetics or psychological factors, such as depression and anxiety), as well as any barriers to managing obesity.
The Three Pillars
To manage obesity, patients need support from one or more of what Dr. Wharton calls the "three pillars" of effective long-term weight loss — pharmacotherapy, cognitive-behavioural therapy and bariatric surgery. All three interventions temper the cascade of neurochemicals that are so intent on putting the weight back on.
Dr. Sasha High, medical director of the High Metabolic Clinic in Mississauga, was pleased to see the recognition of behavioural tools as a means to support a healthy lifestyle included in the guideline.
“For decades, the medical advice to patients with obesity was to "improve your lifestyle" or "eat less, exercise more" — as though, telling patients to have a healthier lifestyle is an intervention. The guideline outlines specific interventions (self-monitoring, challenging intrinsic bias, identifying wanting, developing restraint thoughts, encouraging self-efficacy, etc.) that result in long-term health behaviours by equipping patients with tools and strategies. The healthy lifestyle in and of itself is not the intervention, it is the result of the interventions,” said Dr. High, who was not involved in the guideline’s development.
The guidelines also recognize the role of physical activity in wellness, pointing out that consistently, randomized control trials have linked physical activity with a lower prevalence of cardiovascular risk factors (e.g., high blood pressure, LDL-cholesterol [LDL-C], triglycerides, glucose and low HDL-cholesterol ([HDL-C] levels) and a lower incidence of chronic disease (e.g., type 2 diabetes, cardiovascular disease, certain types of cancer).
Dr. High called the guideline “a big step forward in recognizing that obesity is a complex medical condition.” She says the emphasis on the genetic susceptibility, hormonal control of energy regulation and brain's role in obesity is particularly important because it takes the blame off of the patient.
Dr. High also appreciates the redefinition of obesity as excess adipose tissue causing impairment to health or function. “That means obesity isn't defined by body size. There are individuals with larger bodies who are very healthy. And individuals with smaller bodies who have adiposity-related medical complications. This takes the focus off of esthetics and puts it onto health.” she said.
Over the past three decades, the prevalence of obesity has steadily increased throughout the world, and in Canada, it increased threefold since 1985. Notably, severe obesity has increased more than fourfold and, in 2016, affected an estimated 1.9 million Canadian adults. Given these numbers, a sizable percentage of all practising primary care practices will have patients with obesity. In many practices, patients who are overweight and have obesity may form the majority of the practice. Given the numbers, said Dr. Wharton, it is imperative that physicians understand better approaches to assess and manage are much needed.
“This is the situation facing us now and that is why it is so important that physicians understand increased knowledge of the disease state and better approaches to assess and manage obesity are available. These patients desperately need their doctor to be their partner in managing this disease,” said Dr. Wharton.
With more than 60 co-authors, including physicians, researchers, family doctors, mental health experts, and patients, the guideline was developed in conjunction with the Canadian Association of Bariatric Physicians and Surgeons and Obesity Canada, a non-profit research and advocacy group. Those with competing interests, including Dr. Wharton who is the medical director of a weight loss clinic and member of drug company advisory councils, listed them in the guidelines.
Clinical practice guideline transcript
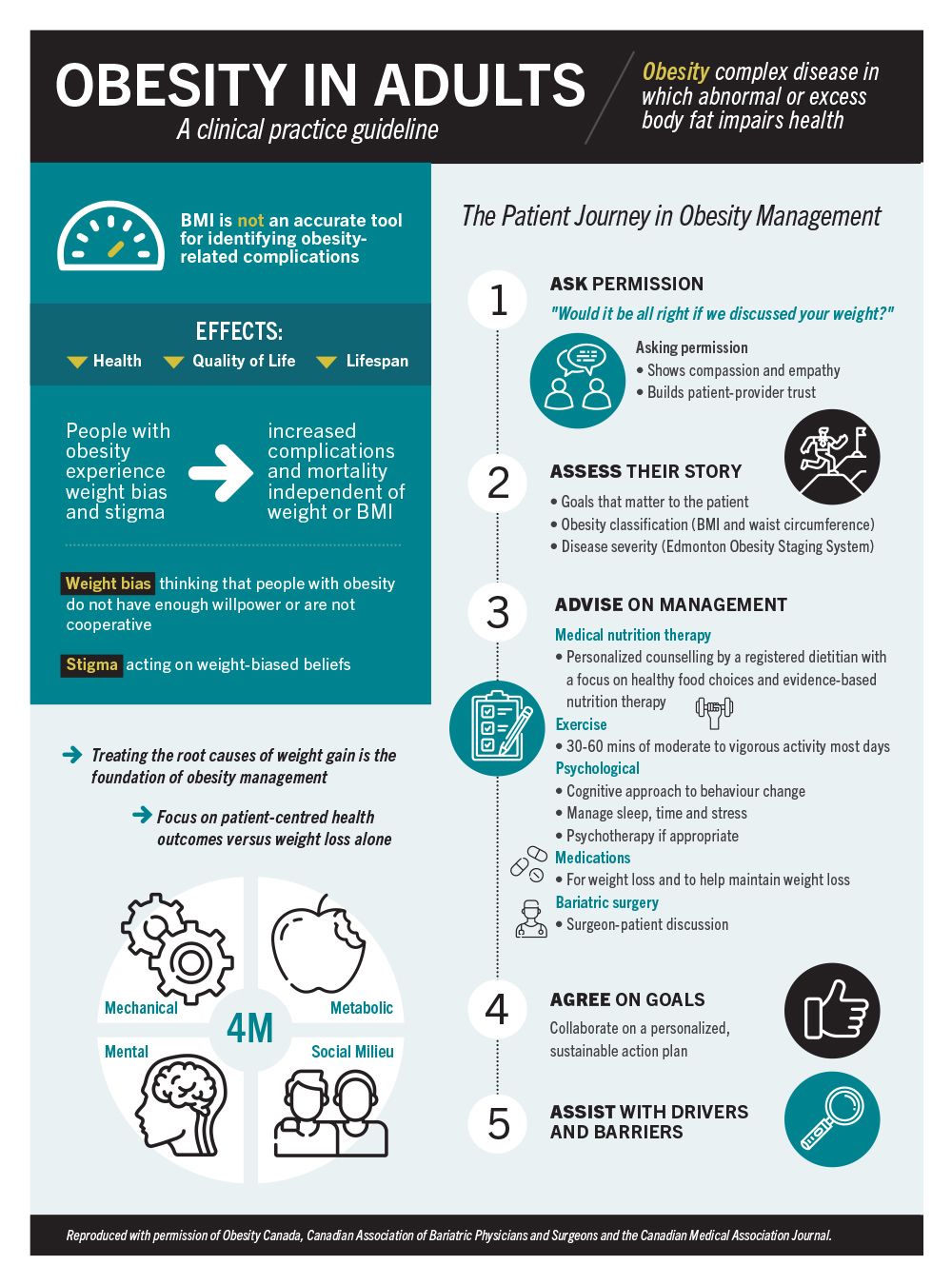
Obesity in Adults
A clinical practice guideline
Obesity: complex disease in which abnormal or excess body fat impairs health.
BMI is not an accurate tool for identifying obesity-related complications.
Obesity effects health, quality of life and lifespan.
People with obesity experience weight bias and stigma, which can result in increased complications and mortality independent of weight or BMI.
Weight bias: thinking that people with obesity do not have enough willpower or are not cooperative.
Stimga: acting on weight-biased beliefs.
Treating the root causes of weight gain is the foundation of obesity management.
Focus on patient-centred health outcomes versus weight loss alone.
The four M’s: Mechanical, Mental, Metabolic and Social Milieu.
The Patient Journey in Obesity Management
- Ask Permission
"Would it be all right if we discussed your weight?"
Asking permission- Shows compassion and empathy
- Builds patient-provider trust
- Assess Their Story
- Goals that matter to the patient
- Obesity classification (BMI and waist circumference)
- Disease severity (Edmonton Obesity Staging System)
- Advise on Management
Medical nutrition therapy- Personalized counselling by a registered dietitian with a focus on healthy food choices and evidence-based nutrition therapy
Exercise
- 30-60 minutes of moderate to vigorous activity most days
Psychological
- Cognitive approach to behaviour change
- Manage sleep, time and stress
- Psychotherapy if appropriate
Medications
- For weight loss and to help maintain weight loss
Bariatric surgery
- Surgeon-patient discussion
- Agree on Goals
Collaborate on a personalized, sustainable action plan - Assist with Drivers and Barriers
Reproduced with permission of Obesity Canada, Canadian Association of Bariatric Physicians and Surgeons and the Canadian Medical Association Journal.




