











But Choosing Wisely Canada says more needs to be done
As the limits of Canada’s health care systems are being tested by COVID-19 and its sustainability is worrying Canadians, a new report looking at trends over time finds clinicians, patients, researchers and policymakers are making progress in reducing the provision of low-value care.
The overuse of health care, or low-value care, offers little to no benefit to patients and can even cause harm, including side effects, unnecessary exposure to radiation, a cascade of more testing, stress and anxiety, among other things. For Canada’s health systems, overused tests and treatments can increase wait times for people who need care, take up patients’ and clinicians’ time, and waste limited health resources.
This new joint report from Choosing Wisely Canada and the Canadian Institute for Health Information — a follow-up to their 2017 Unnecessary Care in Canada report — provides updated and expanded information on the overuse of tests and treatments in Canada. The earlier report found up to 30 percent of tests, treatments and procedures performed in Canada were potentially unnecessary.
The Overuse of Tests and Treatments in Canada report examines the overuse of 12 selected tests and treatments by looking at trends and variation in use across the country from 2014/15 to 2019/20. (Data from 2020/21 was not part of the trend analysis because it is not fully understood how COVID-19 changed the provision and use of health services).
To achieve widespread change, system-level changes are needed, in addition to continued efforts from front-line clinicians and patients.
Over a five-year period, the overuse of eight out of the 12 tests and treatments decreased by 10 percent or more. This represents a reduction of about 826,000 tests, treatments and procedures that would not have benefited patients, including:
- 698,000 fewer unnecessary prescriptions and other treatments;
- 115,000 fewer low-value X-rays, CT scans, MRIs and preoperative tests; and
- 13,000 fewer unnecessary surgical procedures.
“The results are encouraging, but overuse remains an issue and further reductions in low-value care are both possible and necessary,” said Dr. Wendy Levinson, Chair of Choosing Wisely Canada during a webinar announcing the results of the progress report. To achieve widespread change, she said system-level changes are needed, in addition to continued efforts from front-line clinicians and patients.
“Now more than ever, we really need to accelerate work on reducing overuse on low-value care and free-up limited resources to transfer them to where they are absolutely needed,” she said.
The biggest decreases since the 2017 report was produced were: physical restraints in long-term care (decrease of 47 percent;) knee arthroscopy in adults aged 60 and older (decrease of 46 percent) and potentially inappropriate use of antipsychotics in long-term care — decrease of 26 percent).
This report provides examples of actions that have been taken to reduce the overuse of these 12 tests and treatments. These actions may help explain trends and give clinicians, decision-makers and policy-makers ideas for making further reductions.
The report also gauged the Canadian public’s perception of overuse. In 2022, about one in five (19 percent) Canadians reported a test or treatment they did not feel was necessary for their health was recommended to them. This has declined compared with 25 percent in 2019 and 30 percent in 2017.
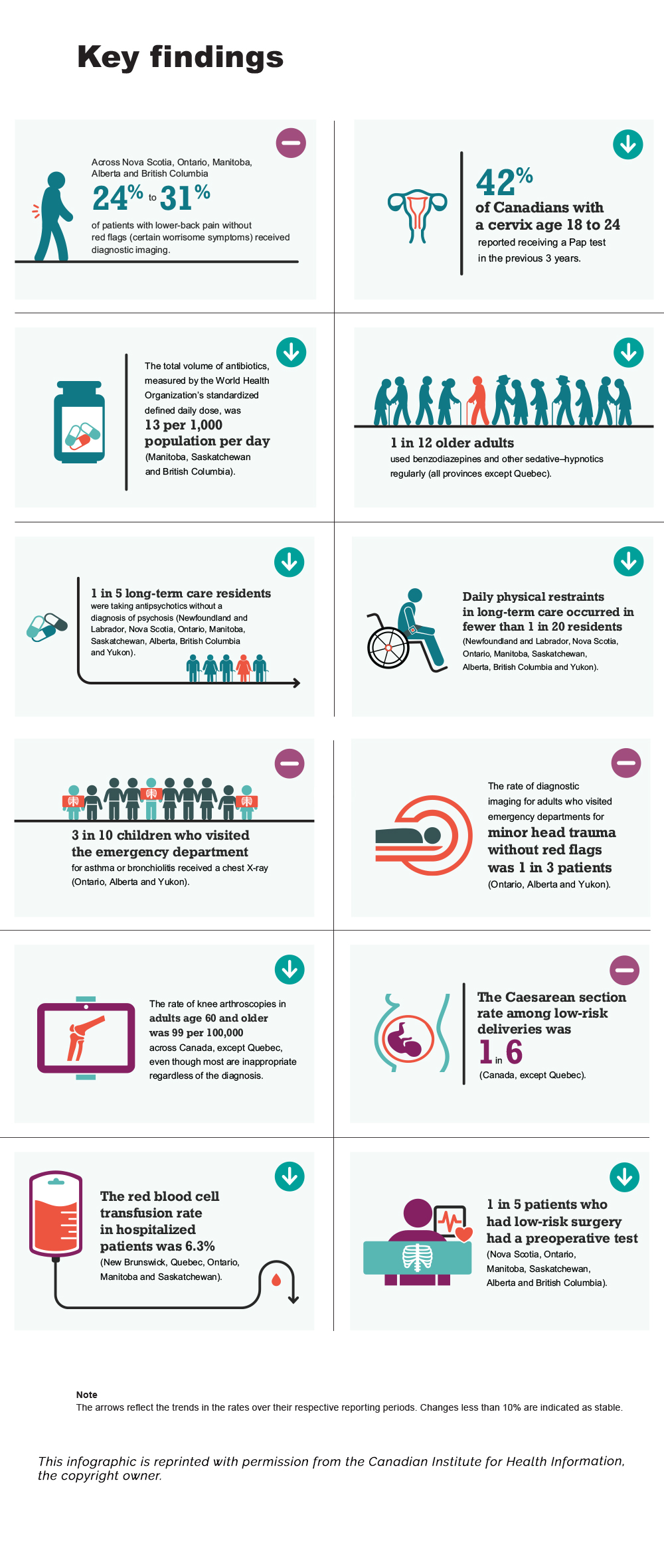
Key Findings infographic transcript
Key Findings
- Stable: Across Nova Scotia, Ontario, Manitoba, Alberta and British Columbia 24% to 31% of patients with lower-back pain without red flags (certain worrisome symptoms) received diagnostic imaging.
- Decrease: 42% of Canadians with a cervix age 18 to 24 reported receiving a Pap test in the previous 3 years.
- Decrease: The total volume of antibiotics, measured by the World Health Organization’s standardized defined daily dose, was 13 per 1,000 population per day (Manitoba, Saskatchewan and British Columbia).
- Decrease: 1 in 12 older adults used benzodiazepines and other sedative–hypnotics regularly (all provinces except Quebec).
- Decrease: 1 in 5 long-term care residents were taking antipsychotics without a diagnosis of psychosis (Newfoundland and Labrador, Nova Scotia, Ontario, Manitoba, Saskatchewan, Alberta, British Columbia and Yukon).
- Decrease: Daily physical restraints in long-term care occurred in fewer than 1 in 20 residents (Newfoundland and Labrador, Nova Scotia, Ontario, Manitoba, Saskatchewan, Alberta, British Columbia and Yukon).
- Stable: 3 in 10 children who visited the emergency department for asthma or bronchiolitis received a chest X-ray (Ontario, Alberta and Yukon).
- Stable: The rate of diagnostic imaging for adults who visited emergency departments for minor head trauma without red flags was 1 in 3 patients (Ontario, Alberta and Yukon).
- Decrease: The rate of knee arthroscopies in adults age 60 and older was 99 per 100,000 across Canada, except Quebec, even though most are inappropriate regardless of the diagnosis.
- Stable: The Caesarean section rate among low-risk deliveries was 1 in 6 (Canada, except Quebec).
- Decrease: The red blood cell transfusion rate in hospitalized patients was 6.3% (New Brunswick, Quebec, Ontario, Manitoba and Saskatchewan).
- Decrease: 1 in 5 patients who had low-risk surgery had a preoperative test (Nova Scotia, Ontario, Manitoba, Saskatchewan, Alberta and British Columbia).
Note: The arrows reflect the trends in the rates over their respective reporting periods. Changes less than 10% are indicated as stable.
This infographic is reprinted with permission from the Canadian Institute for Health Information, the copyright owner.




